.png)




12 billion workdays are lost every year due to mental health conditions, according to the World Health Organization. Not because support does not exist, but because it keeps arriving after the damage is already done. That is the crisis-only trap, and high-stress workforces are paying the price.

The Reality of High-Stress Workforces
When people ask what the most stressful occupations are, the standard list appears: surgeons, soldiers, and air traffic controllers. But that framing misses the larger problem.
The most stressful occupations span entire industries:
- Healthcare workers managing 12-hour shifts, patient mortality, and chronic understaffing
- First responders absorbing trauma as a daily job requirement
- Construction workers navigating physical danger, tight deadlines, and financial volatility
- Corporate professionals in finance, legal, and executive roles facing relentless accountability and decision fatigue
What unites these roles is not just that the work is hard. The stress is structurally embedded. Long hours, emotional exposure, high responsibility, and low autonomy do not create occasional bad days; they create continuous psychosocial risk. Research confirms that chronic role overload and lack of decision latitude are among the strongest predictors of poor mental health outcomes.
What Is Psychological Safety at Work (And Why It Matters)
What is psychological safety at work? Harvard professor Amy Edmondson defines it as a shared belief that team members will not be punished for speaking up, asking questions, or admitting mistakes.
In practice, it is the difference between a nurse flagging early burnout versus silently pushing through until collapse. When psychological safety is absent, early mental health signals go unreported and unaddressed.
A study found that organizations with strong psychosocial safety climates had significantly lower rates of psychological injury and depression. The safety culture itself functions as a prevention mechanism, yet most well-being programs never address it at all.
The Problem with Crisis-Only Mental Health Models
83% of US employees report work-related stress, according to the American Institute of Stress. Yet the dominant workplace response remains built around the crisis moment: the breakdown, the leave of absence, the emergency referral.
Crisis-only models typically include reactive counseling, EAP hotlines triggered after distress becomes unmanageable, and return-to-work programs that manage the aftermath rather than prevent it. The structural failure is one of timing. By the time a healthcare worker calls a crisis line, they have likely been accumulating unaddressed stress for months.
These models treat symptoms, not causes. A burned-out ICU nurse gets counseling sessions and returns to the same understaffed ward. The system resets, ready to catch the next breakdown.
Occupational Stress Is Continuous, Not Episodic
The National Institute for Occupational Safety and Health defines occupational stress as harmful responses that occur when job demands do not match a worker's capabilities or resources.
Its drivers include excessive workload, low control, poor management, and role ambiguity, none of which are sudden. A first responder does not develop PTSD from one call. A corporate lawyer does not burn out from one late night.
Chronic stress progressively impairs cognitive function and emotional regulation before any visible crisis emerges. In high-stakes industries, that degradation has real consequences: diagnostic errors, safety incidents, and compromised decision-making. Treating occupational stress as episodic means organizations are always responding to a late-stage problem.

Why Traditional Employee Well-Being Programs Fall Short
The employee well-being program market is worth billions. Mindfulness apps, wellness stipends, resilience workshops. Most organizations have several. Most are not working. Research shows that traditional Employee Assistance Programs often see utilization rates between 3% and 10%, highlighting a major gap between availability and actual use.
The reasons are predictable: programs require a self-aware, motivated, non-overwhelmed employee to initiate, which is precisely what a burned-out worker is not. They are also disconnected from the workflow generating the stress. A meditation app on a personal phone is not a solution; it is an add-on.
The WHO's 2022 guidelines on mental health at work are explicit: interventions must address organizational risk factors, not just build individual resilience. Programs that skip this step are not wellbeing solutions. They are liability management tools.
The Missing Link: Early Intervention and Proactive Support
Early intervention means identifying stress signals before they escalate. Every dollar invested in early mental health support yields approximately four dollars in improved productivity and reduced absenteeism.
Proactive support requires three things crisis models lack:
- Detection mechanisms that do not depend solely on self-reporting
- Psychological safety that allows employees to signal distress without fear
- Continuous monitoring rather than reactive response
The WHO guidelines are direct: organizations are responsible for preventing risks at the source, not merely treating outcomes. That reframes mental health from HR's crisis list to organizational design.
A Better Model for High-Stress Workforces
Effective mental health infrastructure for high-stress environments rests on four pillars:
- Continuous monitoring using behavioral and engagement signals to surface patterns early
- Manager training to recognize stress indicators and normalize mental health conversations
- Culture-first design where psychological safety is built into how teams operate, not bolted on as a benefit
- Embedded support integrated into workflow rather than offered as a standalone program
Research shows that organizational-level workplace interventions, which target working conditions and psychosocial factors, consistently improve employee mental health outcomes such as stress, burnout, and well-being. The system must change, not just the employee.
Conclusion: The Cost of Waiting for the Crisis
Crisis-only mental health care is not a safety net. It is a cleanup crew. For workforces where stress is chronic, systemic, and predictable, it is not enough.
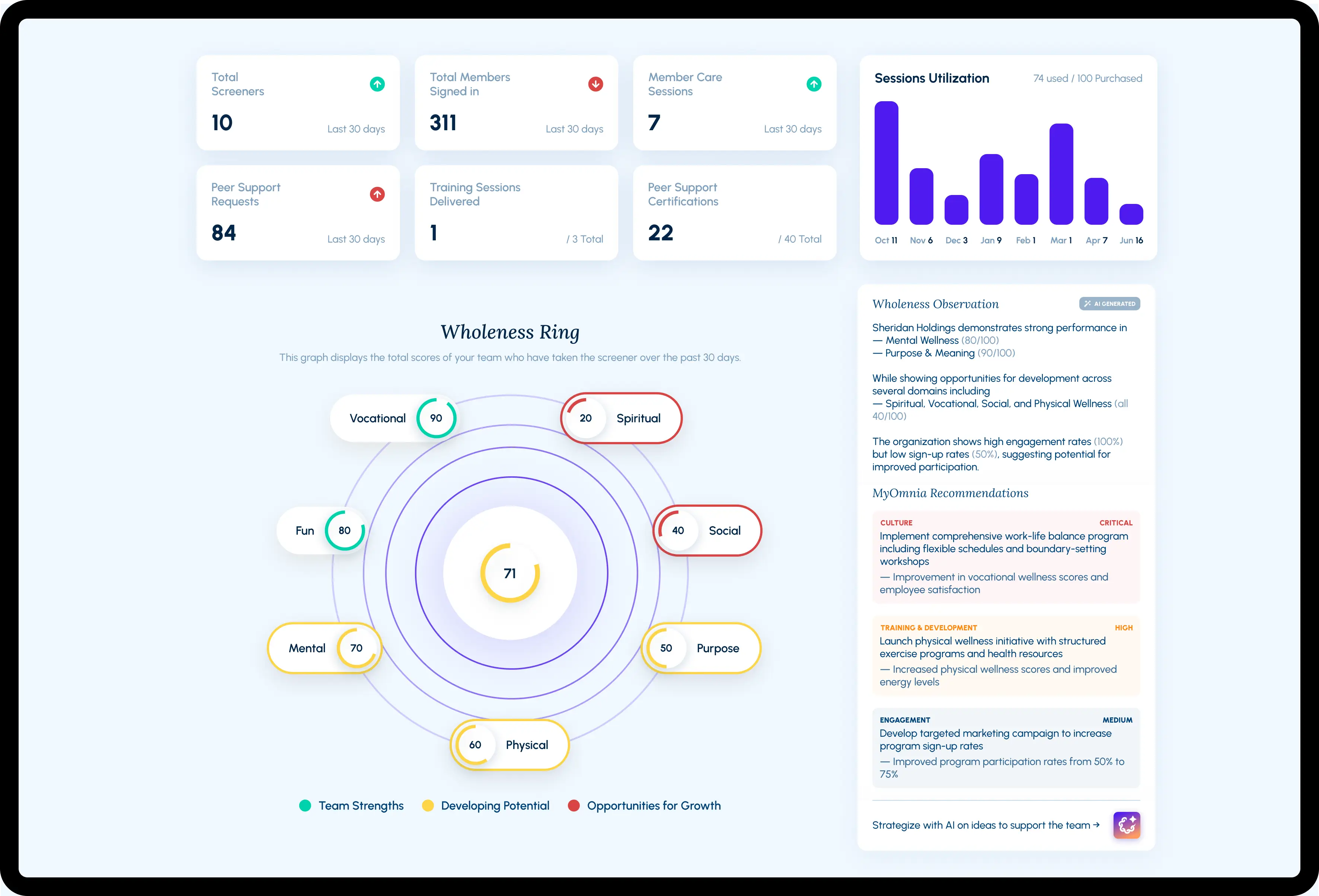
MyOmnia is built for that gap. As an early detection and workforce mental health infrastructure platform, MyOmnia moves organizations from reactive response to continuous, embedded support, identifying risk signals before escalation, building psychological safety, and giving HR leaders the system-level visibility they have always needed.
High-stress work is not going away. The question is whether your mental health model is designed for the work your people are actually doing, or for the crisis that happens when it finally breaks them.